1·
7 months agoThanks! I’ll at it when I get time. I really hadn’t heard of other sites besides thingiverse, and I am yet unaware of any nuances, issues or controversies about it.
Thanks! I’ll at it when I get time. I really hadn’t heard of other sites besides thingiverse, and I am yet unaware of any nuances, issues or controversies about it.
Yeah, the 15w charging is only iPhone, and fast charging doesn’t seem to work – i think because of overheating mostly from my experience. This current setup the charger is closer to my phone than other setups, so I may try it, maybe it fast charging will work, but I don’t have my hopes up.
Hopefully with Qi2 these android users are natively included.
Edit: fast charging still doesn’t work with magsafe
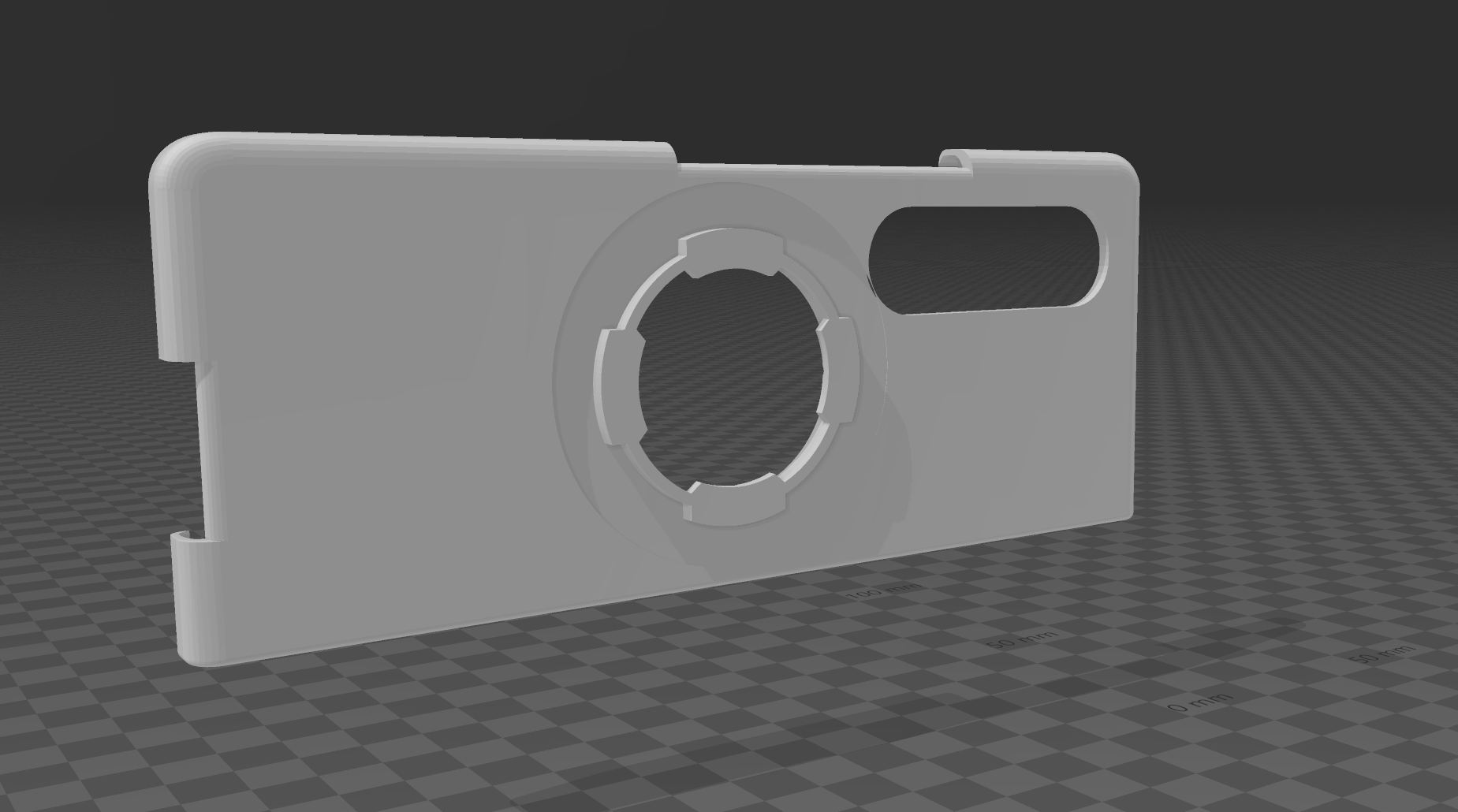
This is just a screenshot… Here’s the STL https://www.thingiverse.com/thing:6354529. I have 3M trasnfer tape that I’ll use to hold it only my phone, which is basically the same sort of stuff that holds my current Spigen phone case on my phone. I’m not sure I’d trust a plastic case on this phone without some sort of adhesive the way the phone is designed. This is essentially just half the case for the back of the folding phone (The front portion, which is made by Spigen, hold the s-pen, which I use somewhat regularly). Hopefullly this prints well and actually works well as far as locking onto quadlock mounts and magsafe with charging working (I use magsafe charging and accessories currently with an adapater – I would expect this to work better since it’d be thinner than my current setup.
I love this. This would make it easier. I can use the exact same cone to “cut” the case. I’ll also be able to perfectly center the cone on the mag quad adapter (not sure if the stl has is 100% centered or not, but this way I can get it perfect.
I’ll play with this. Probably won’t have time for a few days, my days are busy. I tried using sphere deletion in blender yesterday, and it was a bit tough since it was my first time using any 3d design software.
I think this is probably the best suggestion for how to accomplish this, and I’ll be able to focus on doing it soon.
Thanks- I’ll check it out! I liked how simple TinkerCAD felt, and was hoping to use it, if I can, that’d be awesome
Something like that last image is exactly what I’m trying to do! I probably could have described it better.
I think it’s probably a bit more complex than I thought, and I’m not sure it’s doable it tinkerCAD (i couldn’t find any way to trim objects…perhaps i’m just missing it). I’m gonna play with windows 3d builder soon when I get a chance I think.
I’ll check it out. I liked tinkerCad when I used it, but it didn’t seem like there is a way to trim either object to do what I wanted, so I wasn’t sure if it’s the right tool. Maybe a little user error on my end, so I’ll look into it more
Edit: This is as far as I got in Tinkercad/Blender/Automesh – I had trouble actually modifying the shapes in any way in all programs (I am an absolute beginner at this, but I wanna learn and have access to a few different makerbot printers):


This is my crude sketch on what I wanna do.

This is the magquad holder I want to integrate directly into the case.
I don’t wanna stick the holder on my naked phone, and if I put the holder on the case as it is, it will likely be too thick to charge.
Thanks! This sounds a lot, but I wanna try making it. I like modifying things to suit my use, and this sounds like a fun learning endeavor. I’ll perhaps look at OpenSCAD. This sounds similar to some of the information I found on blender (making shapes to delete areas). I need to play with these tools to get more facile at doing this.
I don’t have a picture readily availble at the moment, but the stls are https://www.thingiverse.com/thing:4935721 for the phone case (I just wanna use the right side) and https://www.thingiverse.com/thing:5704716 for the holder. It’s a little more complex than just a magsafe holder, it has a quadlock mount integrated.
https://www.thingiverse.com/thing:4935721 (right cover stl) and https://www.thingiverse.com/thing:5704716 are the two files I’m trying to merge. I’m gonna try playing with windows 3d builder as someone suggested as well
Thanks, I’ll look at it!
I tried with tinkercad, and I struggled. I was again able to align the shapes directly on top of one another, but when it came to modifying the actual shape I could not figure it out- is there a tutorial on adding shapes together or anything, or even carving stuff out?
I looked and couldn’t find anything this specific. It seemed like a much easier tool to use, but I couldn’t figure out how to do what I wanted. I also used
Yes, those are the best fo sure
Nosebleeds can happen and certainly do for some. Nasal hydration helps (for instance, ayr gel in combination with saline spray or irrigations). Ultimately, a good portion of patients that don’t tolerate or fail nasal steroids get surgery.
Azelaetine is fantastic - there’s a lot of patients I prescribe it in conjunction with Flonase. Allergic rhinitis or even just excessive secretions is common in patients with inferior turbinate hypertroph/nasal obstruction, and both meds have a function. They sell it as a combination, actually, but often insurance doesn’t cover the combo.
It would by a sympathetic response from catecholamines – that’s how it constricts; however, I didn’t know that it had been studied and was actually effective in real life until today.
This applies to nasal decongestants (NOT nasal steroids). Nasal decongestants (such as oxymetazoline AKA afrin, or phenylephrine based medications) are vasoconstrictors. They work very well and work very quickly as the vasoconstriction (constricting the blood vessels) which shrinks the inferior turbinates (and any other edematous tissue).
The body responds to chronic vasoconstriction by making more blood vessels. When the nasal tissues have more blood vessels (and I presume are more dense with vessels) it’s harder for the decongestant to work. This is called rebound congestion — conversely, the patients in this scenario will feel they need to use more decongestant since it previously worked so well, but it no longer does. This cycle can be challenging to treat.
For this reason most ENTs, including myself, typically recommend against afrin use for more than 3 consecutive days. I’ve seen who go as long as five, but I’m cautious and would not recommend more than 3 days.
It’s a bit funny, because if you come into my clinic and get an endosocpic exam of the nose and/or throat (i.e. probably around 50%, often more, of my patients on any given day), I will spray afrin and lidocaine into the nose before my examination. The other main thing I use it for is nosebleeds. It’s okay to use it for 3 days during an acute exacerbation of sinusitis, but I don’t really think it’s necessary.
Edit: I forgot to mention nasal steroids. As I said, the above response doesn’t apply to them. We don’t include nasal steroids in this because they have a very slow effect and don’t have the effect of rebound congestion. With few exceptions doing 2 sprays each nostril daily for a very long is fine for almost everybody, and usually helpful. When I prescribe them I recommend patients use them for at least 4 weeks. Once in awhile there are patient that I would be more cautious with prescribing nasal steroids, such as those with a septal perforation, or frequent nose bleeds. Usually it’s a non issue. Tip: when spraying them don’t spray straight back – use your opposite hand and spray towards the eye (i.e. spray with right hand into left nostril, aiming towards left eye).
It csn happen, but the way most ENTs train these days, unlikely. I’ve seen it twice that I recall off the top of my head, but very rare these days.
Most ENTs, including myself, are overly cautious. You’re at a higher risk for symptom recurrence because of under resection.
That being said, I wouldn’t let an oral surgeon or general plastic surgeon touch my family member’s nose (unless they had a very very good reputation). Nothing wrong with their work, I’m just not sure they had the same training and respect for the nose.
True; I, and I’m sure most other physicians would not provide identifiable data in a public forum. If you are having issues with nasal obstruction, alternating or otherwise., best advice is to follow up with your pcm for treatment, possible referral.
The best shitposts are the ones that turn out to be real/useful.


{kind=link}
Natto. Literally the worst, IMO. Even a good number of Japanese folks don’t like it.